Zoological companion animals need rehab, too
Though ZCA species are excellent candidates for rehabilitation, such alternative options for treatment are not often considered

Awareness of the field of veterinary rehabilitation has increased in the past decade. As such, the offering is becoming more common in referral centres, academic institutions, and primary care practices. The field has not been covered in veterinary curricula until recently—particularly with the advent of canine and equine board certifications from the American College of Veterinary Sports Medicine and Rehabilitation (ACVSMR) (vsmr.org). The college was established to meet the needs of athletic, working, and companion animals that are recovering from surgery or have debilitating arthritis, neurologic impairments, or other mobility disorders.
Outside of traditional species, there is a need for this growing field within veterinary medicine. Notably, zoological companion animal (ZCA) species are excellent candidates for rehabilitation; however, for these animals, alternative options for treatment (including rehabilitation) are not often considered.
When clinicians are determining treatment of ZCA patients, a comprehensive mobility assessment is critical, as the ultimate rehabilitation plan will be generated specific to the patient’s diagnosis, sources of pain, and functional limitations. The comprehensive assessment of a mobility impairment can be broken down into four major categories: history and signalment, gait observation, physical examination, and recommended diagnostics.
History/signalment
When considering the categories of differentials for an animal’s mobility impairment, species, age, sex, season, breeding status, and husbandry are each important pieces to the diagnostic puzzle.
Causes for almost any disease can be found in the DAMNITV acronym scheme:
- Degenerative
- Anomalous
- Metabolic
- Neoplastic/Nutritional
- Inflammatory/Infectious/Immune/Idiopathic/Iatrogenic
- Traumatic/Toxic
- Vascular
An animal’s age, for example, aids in the ordering of differential diagnoses, with developmental and nutritional etiologies being more common in immature animals and degenerative and neoplastic etiologies being overrepresented in older animals. Another example is intact male animals often being overrepresented for trauma.
It is necessary, as well, for veterinarians to be mindful of species-specific differentials based on signalment, such as male castrated continental giant breed rabbits being overrepresented for femoral condylar fractures,1 and ferret lymphoma, which can be seen in all ages with no sex predilection.
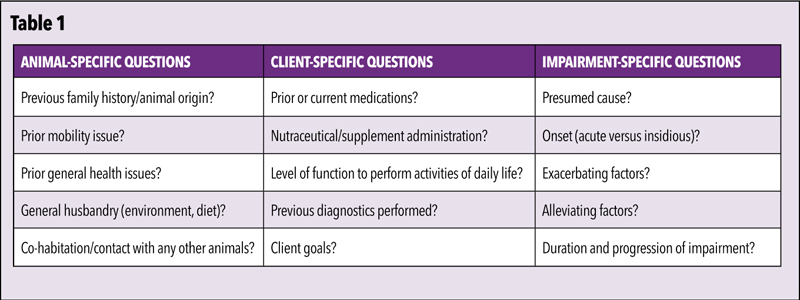
Important history information to obtain for ZCA species comprises specific knowledge about the animal, the client, and the appreciated mobility impairment itself. Table 1 contains a list of relevant questions when obtaining a thorough history for ZCA patients with a mobility impairment. This list, however, is not comprehensive for all species-specific details (i.e. last shed, breeding/laying history, etc.), and a complete husbandry evaluation should be performed in addition.
The impairment-specific questions are crucial when correlating history to the differential diagnoses, as the onset and progression of clinical signs varies significantly between categories. For example, degenerative and neoplastic etiologies typically begin with an insidious onset and gradual progression; trauma, however, occurs suddenly with significant and persistent clinical signs.
As a general word of caution, while inquiring about a client’s identification of a mobility impairment, it is important to remember this question may be misinterpreted. For example, an owner describing an issue with their pet’s ‘left forelimb’ may be referring to their own left instead of the animal’s left. Likewise, ‘favouring’ a limb could mean either this is the preferred limb to bear weight or, rather, this is the limb the pet is treating gently to avoid further injury. To obtain an accurate report, owner-recorded videos of the animal navigating its home environment are recommended. Client service representatives (CSRs) can help facilitate this process at the time the appointment is made.
Gait/Flight observation
The primary goals of observing an animal’s gait and/or flight are to ascertain the limb(s) affected, the severity, and whether the impairment is neurologic, orthopedic, or from another source. In short, the three main reasons for abnormal movement can be due to pain, neurologic pathology, or a loss of a mechanical apparatus (i.e. fibrotic contracture, arthrodesis).
Gait abnormalities from neurologic dysfunction vary based on the underlying pathology and can be categorized as paresis (partial loss of voluntary movement), ataxia (incoordination), and/or neurogenic (‘root signature’) lameness. Upper motor neuron (UMN) and lower motor neuron (LMN) paresis differ in their appearance, with UMN lesions commonly characterized by spasticity and increased muscle tone, and LMN lesions appearing flaccid with decreased muscle tone. Ataxia, if present, is inherently UMN in nature and will not result from orthopedic disease, nor LMN lesions. General proprioceptive ataxia can manifest as knuckling over, scuffing feet, limbs crossing midline, and/or abnormal base-wide/narrow gait.
For quadrupeds, lameness assessment is similar to the principles applied in canids and equids. Weight-bearing forelimb lameness appears as a head nod, with the head lifting up when the lame limb enters stance phase (Video 1). Meanwhile, weight-bearing pelvic limb lameness is characterized by a hip hike or pelvic tilt away from the lame limb and toward the normal limb. These compensations result from the animal’s effort to distribute as much body weight as possible away from the painful limb.
In ZCA patients, ferrets can be challenging to assess. When one pelvic limb is painful, the animal can appear paraparetic, as it is difficult to elevate the length of its body on one pelvic limb alone (Video 2). Likewise, bipedal animals can also pose a challenge, but the principles generally remain the same, with the animal’s pelvis tilting away from lame limb and a drop of the head and/or body when the sound limb is loaded (Video 3).
Another important component of gait assessment is the evaluation of the active range of motion of joints to observe for reduced flexion and/or extension when the animal is ambulating or flying. In rabbits and other hopping species where pelvic limb lameness can be challenging to assess, evaluation of this active range of motion of joints rather than the classic pelvic tilt/hip hike is generally more rewarding.
Additionally, aside from the gait itself, changes in stance, posture, and transitions between positions can be an enlightening source of pathology localization. For example, an animal with stifle pathology can display what is commonly described as a positive ‘sit test’ and refrain from full stifle flexion when sitting or laying down; likewise, an animal with a bilateral pelvic limb lameness may overcompensate with the thoracic limbs to pull themselves up to a stand.
In avian patients, when evaluating for more subtle flight abnormalities, it is recommended to assess the bird when initiating flight, as this is the most energetically demanding component of flying and may elucidate an otherwise imperceptible sign.
As stated previously, owner-filmed videos can be particularly helpful when assessing ZCA species. This permits evaluation in the absence of confounding factors, including the risk of escape and fear/anxiety induced gait and flight alterations (i.e. crouched, rapidly navigating to the closest hiding place), and also allows for assessment in slow motion.
Physical (neuromusculoskeletal) exam
The goal of a neuromusculoskeletal examination is to supplement the general physical exam and to localize the mobility issue to a specific anatomic location. It is important to maintain a consistent, systematic approach, and to also perform this assessment on normal patients, as this can help to establish familiarity with expected species-specific nuances. For example, some unexpected (relative to a normal canine exam) but normal findings include an inconsistent-to-absent panniculus reflex in rabbits, as well as reduced carpal flexion with a capsular end-feel in guinea pigs. It is only through consistent palpation of both normal and abnormal animals in a veterinarian’s primary species of interest that one will achieve a greater degree of confidence when a true abnormal finding is identified.
A recommended systematic approach to a neuromusculoskeletal exam begins with palpation from distal to proximal, including long bones, soft tissues, and joints, as well as a targeted neurologic assessment. Articular assessment consists of evaluation of crepitus, range of motion, effusion, pain, and instability. The grating sensation of crepitus, indenting softness of effusion, and laxity of instability are largely similar across species, but can be challenging to appreciate in more mildly affected cases, or in small species and in patients with overlying soft tissue structures, fur, or feathers.
Normal reference ranges for joint range of motion are not reported for ZCA species. As such, the examiner typically must rely on comparison to the contralateral limb or prior experience in bilaterally affected cases (hence, the merits of routinely examining normal animals). Joint range of motion can be evaluated using a goniometer for a more objective assessment and by utilizing the subjective finding of joint end-feel.
Briefly, end-feel describes what is limiting joint range of motion. The described end-feels vary in their description by source, but largely consist of:
1) Firm and yielding (joint capsule, tendon, or ligament)
2) Hard and unyielding (bone, fibrotic contracture)
3) Muscle spasm
4) Soft tissue approximation (muscles, soft tissue swelling)
5) Empty (unable to reach end feel due to pain)
End-feels can aid the examiner in the determination of normal versus abnormal in the absence of reported joint range of motion references. For example, in the authors’ experience, most ZCA species have a soft tissue approximation end-feel on full elbow flexion with the muscles of the brachium abutting those of the antebrachium restricting any further motion. Thus, if the examiner instead identifies a hard end-feel on elbow flexion, this should raise concern for elbow osteoarthritis, among other less common differentials.
Evaluating pain, while critical, is among the most challenging and subjective components of a mobility assessment. This is particularly true for prey species, as these creatures instinctively mask pain. Thus, it is wise for veterinarians to become familiar with species-specific signs of pain and respective evaluation tools (including facial grimace scales) that are available for some small mammal species. When needed, light anxiolytic sedation can help dampen anxiety to facilitate examination. Heavier sedation with analgesia can be administered to more painful animals with the limitation this will hinder pain localization.
A targeted neurologic assessment (in addition to the evaluation of paresis and ataxia already performed with gait assessment) should include evaluation of postural reactions, abbreviated spinal reflex assessment (flexor withdrawals +/- patellar reflexes where possible), and spinal/paraspinal palpation. Postural reactions in ZCA species can typically be assessed with hopping response testing, whereby the examiner lifts a limb off the ground and shifts the patient’s weight laterally while interpreting its ability to appropriately reposition the foot, as well as strength and muscle tone on the hopping limb. ‘Wheelbarrow’ testing can also be performed by holding the animal upright and slowly pulling them backwards with their paws/feet on the floor to assess their ability to appropriately reposition. In birds or other animals more resistant to this manoeuvre, this technique may be easiest done by holding the patient stationary and dragging a towel backwards to imitate a treadmill-effect (Video 4). The placing reaction test for proprioception by flipping the foot to place the dorsum on the ground is often unsuccessful in ZCA species.
Soft tissue palpation, at a minimum, should involve assessment of muscle mass, asymmetry, and swelling. Additional components of a soft tissue assessment can include flexibility testing (when warranted), with increased flexibility raising concern for rupture and decreased flexibility representing possible contracture or pain. Primary myotendinous pathology and compensatory muscle pain can also be identified in patients with mobility impairments. This is an important consideration when building a rehabilitation treatment plan.
Sign up for our newsletter
Get all the latest news and features from Veterinary Practice News Canada. Submit your email below to get our twice-monthly newsletter.
Popular Articles
-
1
-
2
-
3
-
4
-
5
Read the Latest Issue

